Pain, Placebo, and the Pipeline to New Drugs
- Published6 Nov 2024
- Author Ailie McWhinnie
- Source BrainFacts/SfN

Like so many disorders of the brain and nervous system, pain has proved difficult to translate from lab discoveries to clinical treatments. Compounds showing promise in animal models often fail to work in humans, and each of those setbacks represents years of preparatory work being lost.
At Neuroscience 2024, the Society for Neuroscience’s annual meeting in Chicago, scientists presented new findings emphasizing the urgent need for new pain drugs — particularly for those with mental health issues — alongside approaches to speed up the discovery-to-drugs pipeline.
Chronic Pain Linked with Drug Use — But Only in Depressed Patients
Researchers at Harvard University found people with chronic pain were more than twice as likely to engage in polysubstance use, using combinations of cocaine, heroin, methamphetamine, and marijuana. Their analysis included data from millions of people in the U.S. who participated in the National Health and Nutrition Examination Survey from 2009 to 2010.
Delving further into this statistic, Nasim Maleki, assistant professor of psychiatry at Harvard Medical School, and her team discovered people with depression on top of chronic pain showed the greatest risk for polysubstance use.
This finding highlights the need for integrated healthcare strategies for chronic pain. With current pain drugs often proving ineffective, people sometimes misuse prescription or recreational drugs — or multiple drugs — attempting to feel better, explains Maleki.
Complicating the challenge is the fact that no major breakthroughs in chronic pain treatment have emerged for decades.
“We can actually block pain quite effectively with categories of drugs,” says Greg Dussor, professor and Chair of the Department of Neuroscience at The University of Texas at Dallas. “It’s just that those drugs create other problems that are as bad, if not worse than, the pain itself. And so developing a selective blocker of pain is really what the big challenge has been.”
Accelerating Drug Development with Human Cell Testing
The drug discovery pipeline is often decades long. The first step is fundamental research on a disorder to understand its root causes. Then, researchers identify potential drug targets and later design therapies, which are screened by testing their effect on cell cultures or in animal models. If a compound shows promise, it undergoes rigorous safety testing before moving to clinical trials. But many compounds show promise in animal models only to fail to perform as well in human clinical trials.
One way to reduce this risk is by introducing human testing earlier in the research process, long before clinical trials. Ethically, scientists cannot use human volunteers at this early stage, but stem cell technology advances allow scientists to grow and test specialized human cells in the lab.
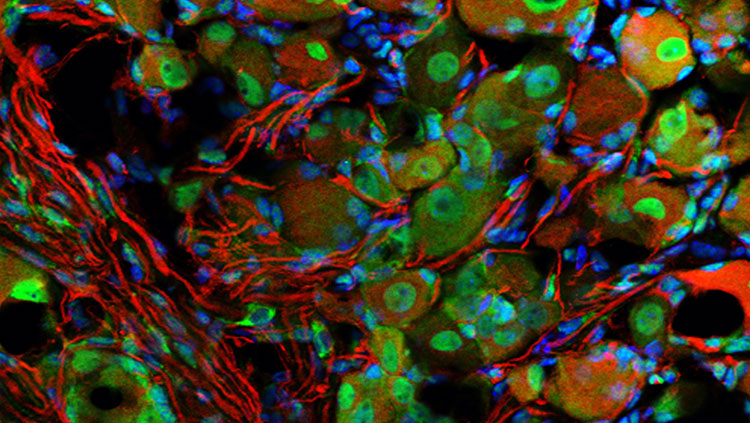
Reprogramming human stem cells into specific cell types is a long and difficult process. But a new method developed by the synthetic biology company bit.bio in Cambridge, U.K., has streamlined the process. Their method reprograms human stem cells into pain-sensing neurons in a single step.
Tony Oosterveen, a principal scientist at bit.bio, says this method reduces cell generation time “from months to days.” If you want to generate neuronal cells to screen drugs, they must act like neurons. For pain-sensing neurons, this means detecting harmful stimuli like extreme temperatures, pressure, and irritating chemicals. bit.bio tested their reprogrammed neurons by subjecting them to well-known pain-inducing chemicals and confirmed this induced neural activity.
“Our sensory neurons offer a very simple model to rapidly test a high number of compounds for their ability to reduce pain,” explains Oosterveen. Generating specialized cells consistently and quickly with technologies like this one allows researchers to easily incorporate human cells at an earlier stage of drug development. The hope, according to Oosterveen, is that adopting such technologies will mean less drugs go on to fail at clinical trials.
Uncovering Circuitry of the Placebo Effect
In clinical trials, participants receive either the drug itself or a placebo, often in the form of a sugar pill. Placebo effect occurs when patients experience relief because they expect to, rather than as a direct result of treatment. Because people taking placebo drugs often experience improvements to their condition, a trialed drug must not only improve symptoms but outperform the placebo effect. “But all new drugs are up against a mechanism we don’t fully understand,” Dussor says.
In a July 2024 study published in Nature by a team at University of North Carolina (UNC), Chapel Hill, researchers induced the placebo effect in mice by placing them in a chamber with a painfully hot side and a relieving cool side. The mice learned to expect relief on the second, cooler side. When both sides of the chamber were made equally hot, the mice still moved to the second side, suggesting their expectation of relief was providing some real relief and the placebo effect was at play.
Brain recordings of the mice showed that as they learned to expect relief, activity in a brain circuit connecting the anterior cingulate cortex, pontine nucleus, and cerebellum increased. The team then used a technique called optogenetics to silence or activate neurons in the circuit. When the circuit was silenced, placebo-trained mice no longer preferred the second side. Conversely, when activated, non-trained mice showed better tolerance to heat, indicating the circuit could mediate pain relief.
“The discovery of the placebo circuit shows the brain contains circuits that can modulate our perception of pain,” explains Grégory Scherrer, associate professor at UNC Chapel Hill School of Medicine who was involved in the study. “We can now target these circuits either with novel drugs or with neurostimulation techniques to develop new treatments for pain.”
For now, failing to outperform placebo is a common hurdle for pain drugs in clinical trials. As evidence of its biological basis builds, perhaps promoting the placebo effect could one day constitute a therapy in its own right.
About the Author

Ailie is a PhD student in neuroscience at the University of Cambridge and a science writer with a particular interest in the intersection of life sciences with history, philosophy and society. Ailie was previously the Public Communications Intern at BrainFacts (Summer/Fall 2024) and editor-in-chief of EUSci and Women in Neuroscience UK.
CONTENT PROVIDED BY
BrainFacts/SfN
References
Chen, C., Niehaus, J. K., Dinc, F., Huang, K. L., Barnette, A. L., Tassou, A., Shuster, S. A., Wang, L., Lemire, A., Menon, V., Ritola, K., Hantman, A. W., Zeng, H., Schnitzer, M. J., & Scherrer, G. (2024). Neural circuit basis of placebo pain relief. Nature, 632(8027), 1092–1100. https://doi.org/10.1038/s41586-024-07816-z
Colloca L. (2019) The Placebo Effect in Pain Therapies. Annu Rev Pharmacol Toxicol. 6(59) 191-211. https://doi.org/10.1146/annurev-pharmtox-010818-021542
Institute for Health Metrics and Evaluation (IHME), (2018). Findings from the Global Burden of Disease Study 2017. IHME. https://www.healthdata.org/sites/default/files/files/policy_report/2019/GBD_2017_Booklet.pdf
World Health Organization. (2023, August 29). Opioid Overdose. https://www.who.int/news-room/fact-sheets/detail/opioid-overdose
What to Read Next

Also In Pain



Trending
Popular articles on BrainFacts.org